Performance Tracker 2023: Adult social care
The government has provided more funding, but the sector may struggle to address unmet need in the face of rising costs and competing priorities.
The government has acknowledged that the availability of publicly funded adult social care* has not been sufficient to meet people’s needs for care and support. It provided a large injection of funding in the autumn statement in 2022 and subsequently. But the adult social care sector faces extensive challenges, including an ongoing workforce crisis, rising costs of providing services and pressure on local authority finances – meaning that even the new level of funding is unlikely to be enough to substantially increase service provision to address the rising levels of unmet and under-met need that have emerged since 2009/10.
Boris Johnson promised to fix adult social care “once and for all” and announced reforms to both the charging model for adult social care and to the wider sector. But the government has abandoned the implementation of charging reforms in this parliament and substantially pared back funding for other reforms. The former decision may have been understandable in the short term, as implementing large-scale charging reforms while adult social care is in crisis would have required far more money than the government was willing to spend. But delay means that it is now more than 11 years since the government-commissioned Dilnot review first recommended a reform to how care is funded, without any meaningful progress having been made.
The result is that many people are still exposed to “catastrophic care costs” and others are denied publicly funded care by a means test that the government has not meaningfully uprated since 2010/11.
The market of private providers who deliver most adult social care remains unstable: despite recent funding increases, average fees simply do not meet operating costs and are below the level that would allow firms to pay social care workers enough to improve recruitment and retention. The government’s proposal that local authorities would “move towards” paying a “fair cost of care” were met with tentative hope in the provider market, only for many to be left disappointed by the government’s decision to delay that reform until October 2025.
As with the NHS, the government is now relying on overseas workers from outside the EU to boost workforce numbers. This has been crucial in filling workforce gaps but is unlikely to be sustainable and can raise ethical concerns, such as exploitation of workers who rely on continued employment to remain in the country. Relying on international staff also does nothing to resolve the fact that social care workers are paid less than workers in comparable sectors – which makes it close to impossible to recruit and retain enough staff and results in high turnover.
This range of problems makes it easy to forget that at its core adult social care should be about empowering people to live “gloriously ordinary lives”. The government’s failure on a range of these issues lets down those who rely on adult social care and is particularly concerning in the context of expected increases in demand.
This chapter looks at the performance of adult social care services that are funded by the state and does not assess the services available to those who pay for their own care.
*Adult social care services provide support to individuals who need it to live independently as well as to their families and carers. Care can be delivered at home (known as domiciliary or home care), in residential or nursing homes, in supported living, in day-care centres, or through using a personal assistant. Care is largely supplied by private or not-for-profit providers and unpaid carers, though local authorities and the NHS also provide some care directly. For those who are eligible for publicly funded care, local authorities are responsible for commissioning and paying for at least some of their care.
Spending remains well above pre-pandemic levels
In response to the Covid-19 pandemic, the government substantially increased the amount it spent on adult social care, with a 7% real-terms increase between 2019/20 and 2020/21. Since then, spending has levelled off, with only a 0.4% real-terms increase in 2021/22* and a 1.6% real-terms increase in 2022/23.
This approach of ‘crisis-cash-repeat’ is ineffective and represents poor value for money. Emergency funding in the winter of 2022/23 offers a good example of its shortcomings. First, government funding was announced and then disbursed late. The Adult Social Care Discharge Fund, worth £500m, was announced in September 2022, already well into the period when the NHS, local authorities and social care providers would have been planning their winter capacity. The £250m of emergency winter pressures funding was not announced until 9 January 2023 – far into the worst of the crisis. 247 Department of Health and Social Care, ‘Oral statement to parliament: New discharge funding and NHS winter pressures’, GOV.UK, 9 January 2023, www.gov.uk/government/speeches/oral-statement-on-new-discharge-funding-and-nhs-winter-pressures Even after announcing the Adult Social Care Discharge Fund in September, it took the government until December to disburse the first tranche – 40% of the total – to councils and the NHS, with the remaining 60% leaving central government coffers in January 2023. 248 Humphries R, ‘Hospital discharge funding: why the frosty reception to new money?’, blog, The Health Foundation, 13 January 2023, retrieved 17 October 2023, www.health.org.uk/news-and-comment/blogs/hospital-discharge-funding-why-the-frosty-reception-to-new-money
Second, the funding came with burdensome reporting requirements. The government required local authorities to detail how they planned to spend all their funding four weeks after it announced allocations. Thereafter, local authorities were expected to provide fortnightly activity reports, with a final report due in May 2023. 249 Department of Health and Social Care, ‘Adult social care discharge fund. Annex B: grant conditions’, 16 March 2023, retrieved 17 October 2023, www.gov.uk/government/publications/adult-social-care-discharge-fund/annex-b-grant-conditions For already under-resourced councils, this represented extra work with little obvious benefit to them.
Third, it is unclear whether the money has even been effective in its stated goal. The funding allocated in 2022/23 was intended to reduce the number of people in hospital who did not need to be there. But evidence that it was effective is mixed. On one hand, in the last week of February 2023, there were on average 13,720 people in hospital per day who were eligible for discharge, compared to 13,545 in the last week of November 2022 – an increase of 1.3%. On the other in the same period in 2021/22, delayed discharges increased by approximately 13%, and in the absence of funding, the level would likely have been higher in 2022/23. However, there is also evidence that while delayed discharge was largely flat in acute hospitals throughout the winter of 2022/23 (as shown in Figure 3.2), that may have been achieved at least in part by shifting people to other parts of the health and care system. Research by Nuffield Trust shows that there was an increase in the number of people delayed in community beds throughout the winter of 2022/23. There were approximately 5,300 people delayed in that setting at the start of November 2022, rising to just over 6,000 in March 2023 – an increase of roughly 13%. 250 Dodsworth E, ‘Growing numbers of delayed discharges from community hospitals’, blog, Nuffield Trust, 10 August 2023, retrieved 17 October 2023, www.nuffieldtrust.org.uk/resource/growing-numbers-of-delayed-discharges-from-community-hospitals As Nuffield Trust says in its analysis: “It is vital that bottlenecks [in acute hospitals] are addressed rather than shifted elsewhere to the detriment of patients stuck in community beds.” 251 Dodsworth E, ‘Growing numbers of delayed discharges from community hospitals’, blog, Nuffield Trust, 10 August 2023, retrieved 17 October 2023, www.nuffieldtrust.org.uk/resource/growing-numbers-of-delayed-discharges-from-community-hospitals
It is fair to say that delayed discharges would likely have been higher in the winter of 2022/23 without the emergency funding, but that the same amount of money could have been spent more effectively to achieve better outcomes than it eventually did.
As an example of how longer-term, more consistent funding might have had better outcomes, we should look at how local authorities and providers actually spent emergency funding. Adult social care capacity is driven predominantly by the number of staff that providers can employ. But short-term funding made it difficult for providers to quickly and sustainably expand the workforce knowing that funding for salaries would run out at the end of winter. 252 Hoddinott S and Davies N, 'Adult social care: Short-term support and long-term stability', Institute for Government, March 2023, www.instituteforgovernment.org.uk/publication/adult-social-care Even when providers were willing to take on more staff, there was a lag between creating a vacancy and employing and training an individual to do the job, meaning that the last-minute funding took a long time to filter through to increased capacity. Interviewees also reported that instead of waiting to fill vacancies, local authorities and providers spent most of the money on measures such as providing staff with one-off bonuses to discourage them from leaving, 253 Institute for Government interview. bringing forward the scheduled national living wage increase, or using expensive agency staff who do not represent good value for money. 254 Institute for Government interview. This may have helped in the short term but will not provide the type of increased stability that longer-term investment in measures such as improved training or career progression might have.
Other examples of ‘crisis-cash-repeat’ also demonstrate poor value for money. The Department of Health and Social Care (DHSC) ran an evaluation of the Workforce Recruitment and Retention Fund, which allocated £462.5m of funding for growing the social care workforce during the pandemic. It found that “the number of staff recruited between the funded period and baseline period is not statistically significant”. 255 Department of Health and Social Care, ‘Workforce Recruitment and Retention Funds: outcomes and findings’, 26 January 2023, retrieved 17 October 2023, www.gov.uk/government/publications/workforce-recruitment-and-retention-funds-outcomes-and-findings/workforce-recruitment-and-retention-funds-outcomes…; Despite little impact on recruitment, there was improved retention, leading to an increase of 2.9 million staff hours compared to baseline. But that expanded capacity was expensive, costing the government £160 per additional hour, 256 Department of Health and Social Care, ‘Workforce Recruitment and Retention Funds: outcomes and findings’, 26 January 2023, retrieved 17 October 2023, www.gov.uk/government/publications/workforce-recruitment-and-retention-funds-outcomes-and-findings/workforce-recruitment-and-retention-funds-outcomes… far above the £10.11 that was the median hourly rate paid to care workers in the independent sector in March 2023. 257 Skills for Care, The state of the adult social care workforce in England, October 2023, retrieved 17 October 2023, p. 117, www.skillsforcare.org.uk/Adult-Social-Care-Workforce-Data/Workforce-intelligence/documents/State-of-the-adult-social-care-sector/The-State-of-the-Adu… The evaluation explicitly pointed to the short-term and last-minute nature of the funding as a reason for its ineffectiveness.
Without extra funding, reforming the charging model for adult social care in 2023 would have been difficult
In 2021, the government launched plans for major reform of adult social care in its People at the Heart of Care white paper
258
Department for Health and Social Care, People at the Heart of Care: Adult social care reform white paper, Cp 560, The Stationery Office, 2021, www.gov.uk/government/publications/people-at-the-heart-of-care-adult-social-care-reform-white-paper
and of the charging model for the sector in the Build Back Better white paper.
259
Department for Health and Social Care, Build Back Better: Our plan for health and social care, Cp 506, The Stationery Office, 2021, www.gov.uk/government/publications/build-back-better-our-plan-for-health-and-social-care
But these plans have since been substantially pared back, with the government delaying plans for charging reform and, in April 2023, reducing funding allocated for other reforms. Those decisions break Boris Johnson’s promise to solve the social care crisis “once and for all”
260
Espadinha M, ‘Prime Minister vows to fix social care crisis’, FT Adviser, 25 July 2019, retrieved 17 October 2023, www.ftadviser.com/pensions/2019/07/25/prime-minister-vows-to-fix-social-care-crisis
and push the question of reform into the next parliament, at the earliest.
The delay in charging reforms will likely be very disappointing to both the users of social care and those who work in the sector. However, interviewees said that the combined pressures of stabilising a market in crisis and implementing a complex set of charging reforms would have been difficult for local authorities, given the resources available to them. 261 Institute for Government interviews. Councils are under-resourced in terms of both funding – with many arguing that the money allocated for charging reforms was far below the amount needed to make them a success 262 County Councils Network, ‘New analysis warns government has ‘seriously underestimated’ the costs of adult social care charging reforms’, press release, 18 March 2022, retrieved 17 October 2023, www.countycouncilsnetwork.org.uk/new-analysis-warns-government-has-seriously-underestimated-the-costs-of-adult-social-care-charging-reforms – and staff and capacity. 263 Care England, ‘Inadequate Funding Undermines Social Care Reforms’, press release, 26 May 2022, retrieved 17 October 2023, www.careengland.org.uk/inadequate-funding-undermines-social-care-reforms A report from Newton and the County Councils Network estimated that local authorities would need to hire an additional 4,300 social workers – an increase of 39% from current numbers – and 700 more financial assessors, an increase of 25%. 264 Newton and County Councils Network, Preparing for reform, 26 May 2022, p. 32, https://futureasc.com/reform The current backlog in care assessments would also have been exacerbated by the government’s charging reforms, which would have generated a large increase in assessments for local authorities to carry out. 265 LaingBuisson, Impact Assessment of the Implementation of Section 18(3) of The Care Act 2014 and Fair Cost of Care: A report commissioned by the County Councils Network, March 2022, p. 7, www.countycouncilsnetwork.org.uk/wp-content/uploads/LaingBuisson-Impact-Assessment-of-Section-183-FCC-FINAL-1.pdf
It is also important to emphasise that charging reforms would not have increased the amount of funding available for the sector, but rather changed the source of that funding. While the improved generosity of the means test would have helped some, reforms would not have changed many of the fundamental issues in the service, such as relatively low pay or care packages that leave many with unmet or under-met needs.
Cost pressures mean that increased funding might not achieve all the government’s objectives
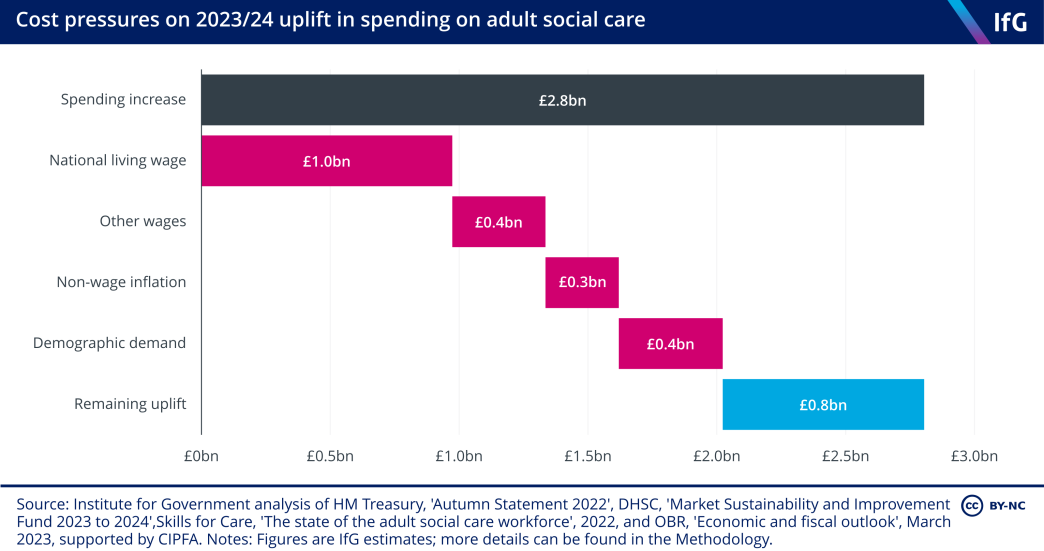
In total, spending on adult social care will rise by approximately £2.8bn between 2022/23 and 2023/24 in cash terms – the largest increase since at least 2009/10. This is a combination of new money announced in the 2022 autumn statement, previously planned changes in spending, and an additional £365m of funding through the Market Sustainability and Improvement Fund (MSIF), 266 Department of Health and Social Care, ‘Market Sustainability and Improvement Fund - Workforce Fund: policy statement', 31 August 2023, retrieved 17 October 2023, www.gov.uk/government/publications/market-sustainability-and-improvement-fund-workforce-fund/market-sustainability-and-improvement-fund-workforce-fun… which the government announced in July 2023. But providers’ cost pressures are severe, so it is unlikely that the funding will achieve its stated objectives.
The sources of these cost pressures are multifaceted. First, a substantial proportion of the social care workforce are paid the national living wage (NLW). The government increased the NLW by 9.7% in April 2023, to compensate low-paid workers for rising inflation. 267 Low Pay Commission, ‘The National Minimum Wage in 2023’, 31 March 2023, retrieved 17 October 2023, www.gov.uk/government/publications/the-national-minimum-wage-in-2023/the-national-minimum-wage-in-2023 The Care Policy and Evaluation Centre estimates that 62.5% of the wage bill in adult social care is spent on staff who are paid the NLW, 268 Hu B, Hancock R and Wittenberg R, Projections of Adult Social Care Demand and Expenditure 2018 to 2038, Care Policy and Evaluation Centre at the London School of Economics, December 2020, p. 9, www.lse.ac.uk/cpec/assets/documents/cpec-working-paper-7.pdf meaning that any increases have a large effect on spending for adult social care. Using this proportion, the 9.7% rise in the NLW will cost providers approximately £1bn in 2023/24.
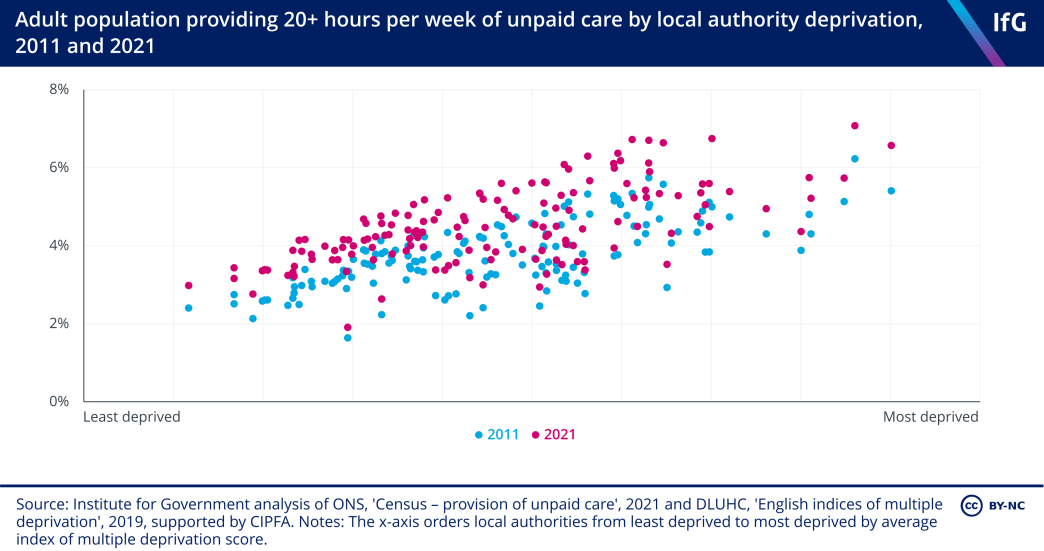
The distribution of those providing large amounts of unpaid care is not even across the country. The more deprived a local authority, the more likely it is that someone living there is providing more than 20 hours per week of unpaid care.